A common spiral-shaped, urease-producing Gram-negative bacterium that colonizes the gastric mucosa; causes chronic gastritis and most peptic ulcers, and is a known risk factor for gastric adenocarcinoma and MALT lymphoma.
Infects roughly half of the world's population and is the leading cause of peptic ulcer disease (over 90% of duodenal ulcers). Identifying and eradicating H. pylori not only heals ulcers (preventing recurrence) but also lowers the risk of gastric cancer (it's classified as a Group 1 carcinogen by WHO).
Often asymptomatic initially. When symptoms occur, chronic dyspepsia is common – gnawing or burning epigastric pain (classically worse when the stomach is empty, e.g. at night), sometimes relieved by eating.
Suspect H. pylori in a patient with an ulcer but no NSAID use (especially a duodenal ulcer in a younger adult). Infection is usually acquired in childhood (more prevalent in crowded, low-sanitation settings) and can persist for decades.
Ulcer complications: GI bleeding (hematemesis, melena, iron-deficiency anemia) or perforation (acute abdomen). Long-standing infection can lead to atrophic gastritis and hence gastric cancer – so weight loss, progressive dysphagia, or other alarm features warrant prompt evaluation.
For patients <60 with dyspepsia and no red flags, follow a test-and-treat approach: perform a noninvasive H. pylori test (urea breath test or stool antigen); if positive, proceed with eradication therapy (if negative, consider other causes or endoscopy).
If alarm features are present or patient is ≥60, skip straight to endoscopy with biopsy for H. pylori testing and to exclude malignancy.
Avoid false negatives: stop PPIs for ~2 weeks and antibiotics for ~4 weeks before testing for H. pylori (acid suppression and recent antibiotics can suppress the bacteria and yield false-negative results).
After treatment, always confirm eradication – usually with a urea breath or stool antigen test ≥4 weeks after therapy (especially important if the patient had an ulcer, MALT lymphoma, or persistent symptoms).
If initial therapy fails, use a salvage regimen with different antibiotics (avoid repeating clarithromycin or metronidazole). Consider culture and sensitivity testing after multiple treatment failures.
Condition
Distinguishing Feature
NSAID-induced ulcer
peptic ulcer with negative H. pylori tests; history of chronic NSAID use (e.g., ibuprofen)
gastrinoma causing massive acid secretion, recurrent ulcers, high gastrin levels
Functional (non-ulcer) dyspepsia
ulcer-like chronic indigestion but normal endoscopy (no ulcer) and no H. pylori
First-line (in regions of low resistance): clarithromycin-based triple therapy – a PPI + clarithromycin + amoxicillin for 14 days (if penicillin-allergic, substitute metronidazole for amoxicillin).
If high local clarithromycin resistance or prior macrolide exposure: use bismuth quadruple therapy – PPI + bismuth subsalicylate + metronidazole + tetracycline for 14 days (an alternative 4-drug regimen is PPI + clarithromycin + amoxicillin + metronidazole).
After completion of therapy, confirm eradication (urea breath or stool test ≥4 weeks later). If H. pylori persists, switch to a salvage regimen using different antibiotics (e.g., levofloxacin- or rifabutin-based triple therapy).
Mnemonic for therapy: CAP = Clarithromycin + Amoxicillin + PPI (triple therapy); PBMT = PPI + Bismuth + Metronidazole + Tetracycline (bismuth quadruple therapy).
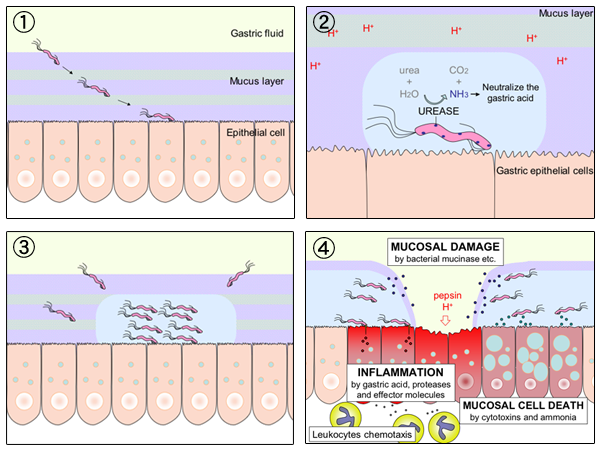
Urease-positive: H. pylori produces urease (ammonia cloud) to alkalinize its surroundings – basis for the urea breath test and rapid urease (CLO) test on biopsy.
H. pylori is implicated in >90% of duodenal ulcers and ~75% of gastric ulcers. An exam tip: an ulcer patient without NSAID use → think H. pylori.
Alarm features suggesting cancer or complicated ulcer: unintentional weight loss, progressive dysphagia, GI bleeding (melena, hematemesis) or anemia, persistent vomiting, or palpable mass → indicate need for immediate endoscopic evaluation.
Ulcer that is refractory (won't heal) despite therapy → suspect treatment failure or an alternate cause (e.g., noncompliance, persistent H. pylori, NSAIDs, Zollinger-Ellison syndrome, or malignancy).
Dyspepsia or ulcer symptoms → check for red flags.
If no alarm features and age <60 → noninvasive H. pylori test (urea breath or stool antigen).
If test positive → treat with eradication regimen; if negative → consider other causes (GERD, functional dyspepsia) or proceed to endoscopy if symptoms persist.
If alarm features or age ≥60 → perform endoscopy with biopsy (for H. pylori detection and to rule out gastric malignancy).
After treatment, perform a test-of-cure (urea breath test or stool antigen) ≥4 weeks later to ensure H. pylori eradication.
Middle-aged adult with burning epigastric pain that improves after meals and wakes them at night; no NSAID use, positive urea breath test → H. pylori–associated duodenal ulcer.
Gastric biopsy showing low-grade MALT lymphoma → treating the H. pylori infection can lead to lymphoma regression.
Patient with long-standing H. pylori gastritis who has new weight loss and early satiety → suspect gastric adenocarcinoma developing (H. pylori as a key risk factor).
Case 1
A 45-year-old man has months of burning epigastric pain that often wakes him at night and is relieved by food.
Diagram illustrating how H. pylori infection leads to gastric ulceration: the bacteria penetrate the mucus layer, produce ammonia (via urease) to neutralize acid, colonize the stomach lining, and cause mucosal damage and inflammation.