Inappropriate, continued ADH release (from pituitary or ectopic source) leading to excess water reabsorption and dilutional hyponatremia (low serum sodium and low plasma osmolality) in a patient with normal volume status (euvolemia).
A common cause of hyponatremia (especially in hospitalized patients) that can lead to serious neurologic symptoms (seizures, coma) if severe. Often tested due to its classic associations (e.g., paraneoplastic small cell lung cancer) and the need to manage sodium carefully to avoid osmotic demyelination.
Often mild or asymptomatic unless serum sodium falls significantly. May cause headache, nausea, gait instability, or in severe cases confusion, seizures, and coma. Physical exam shows no edema or signs of dehydration (patient is euvolemic).
Common triggers: CNS disorders (stroke, hemorrhage, trauma, infections), pulmonary diseases (pneumonia, tuberculosis), malignancies (especially small celllung carcinoma), and various medications (e.g., SSRIs, carbamazepine, cyclophosphamide, MDMA).
Labs: Hypotonic hyponatremia (low serum sodium <135 mEq/L with low plasma osmolality) and inappropriately concentrated urine (Urine Osm >100 mOsm/kg, Urine Na >40 mEq/L) despite normal adrenal, renal, and thyroid function.
Confirm true hyponatremia is hypotonic: check plasma osmolality (will be low in SIADH; if normal or high, evaluate for pseudohyponatremia or hyperglycemia).
Assess volume status or use urine studies to classify hyponatremia: in SIADH the patient appears euvolemic (no edema or orthostasis).
Check urine osmolality and urine sodium: SIADH typically shows Urine Osm >100 mOsm/kg (not maximally dilute) and Urine Na >40 mEq/L (kidneys not sodium-retaining).
Exclude other causes of euvolemic hyponatremia: perform adrenal (cortisol) and thyroid function tests to rule out Addison disease and hypothyroidism.
Identify the underlying cause: review medications, obtain chest imaging (to check for lung tumor), and consider CNS imaging if appropriate, since treating the trigger (tumor removal, stopping offending drug) is key.
Condition
Distinguishing Feature
Hypovolemic hyponatremia
e.g., dehydration, diuretics – patient has volume depletion (dry mucous membranes, orthostasis) and typically low urine Na (<20 mEq/L)
Primary polydipsia
excessive water intake (or low solute diet) – hyponatremia with maximally dilute urine (urine Osm <100 mOsm/kg)
Adrenal insufficiency (Addison disease)
cortisol deficiency causes hyponatremia (with hypotension, hyperkalemia); distinguish by low cortisol levels and response to hormone replacement
Treat the underlying cause (e.g., resect a tumor, discontinue offending drugs, treat CNS injury or infection).
For acute or severe hyponatremia with neuro symptoms (seizures, coma): give hypertonic (3%) saline cautiously to raise sodium ~4–6 mEq/L and alleviate symptoms (avoid overcorrection).
Fluid restriction (≤1 L/day) is first-line for chronic or mild SIADH. Oral salt tablets or increased dietary salt can help raise serum sodium; a loop diuretic may be added to enhance free water excretion.
If hyponatremia is refractory or moderate: consider demeclocycline (induces nephrogenic DI) or vasopressin receptor antagonists (vaptans like tolvaptan) under close monitoring. These are typically second-line due to cost or toxicity.
Correct chronic hyponatremia slowly (≤8–10 mEq/L per 24 hours) to prevent osmotic demyelination (central pontine myelinolysis).
Small cell lung cancer (paraneoplastic ADH secretion) is a classic cause of SIADH on exams.
No peripheral edema in SIADH: excess water intake triggers renal Na+ loss (via ANP), preventing significant fluid overload (patient stays euvolemic).
Giving normal saline doesn't correct SIADH hyponatremia (kidneys will excrete the salt and retain water); use hypertonic saline for severe cases and otherwise restrict fluids.
Severe hyponatremia (e.g., Na <120 mEq/L) or rapid-onset hyponatremia can cause seizures, increased intracranial pressure, or herniation – requires prompt treatment with hypertonic saline.
Overly rapid correction of sodium (>10 mEq/L in 24 hours) can lead to osmotic demyelination syndrome (central pontine myelinolysis) – characterized by irreversible neurologic damage (e.g., quadriplegia).
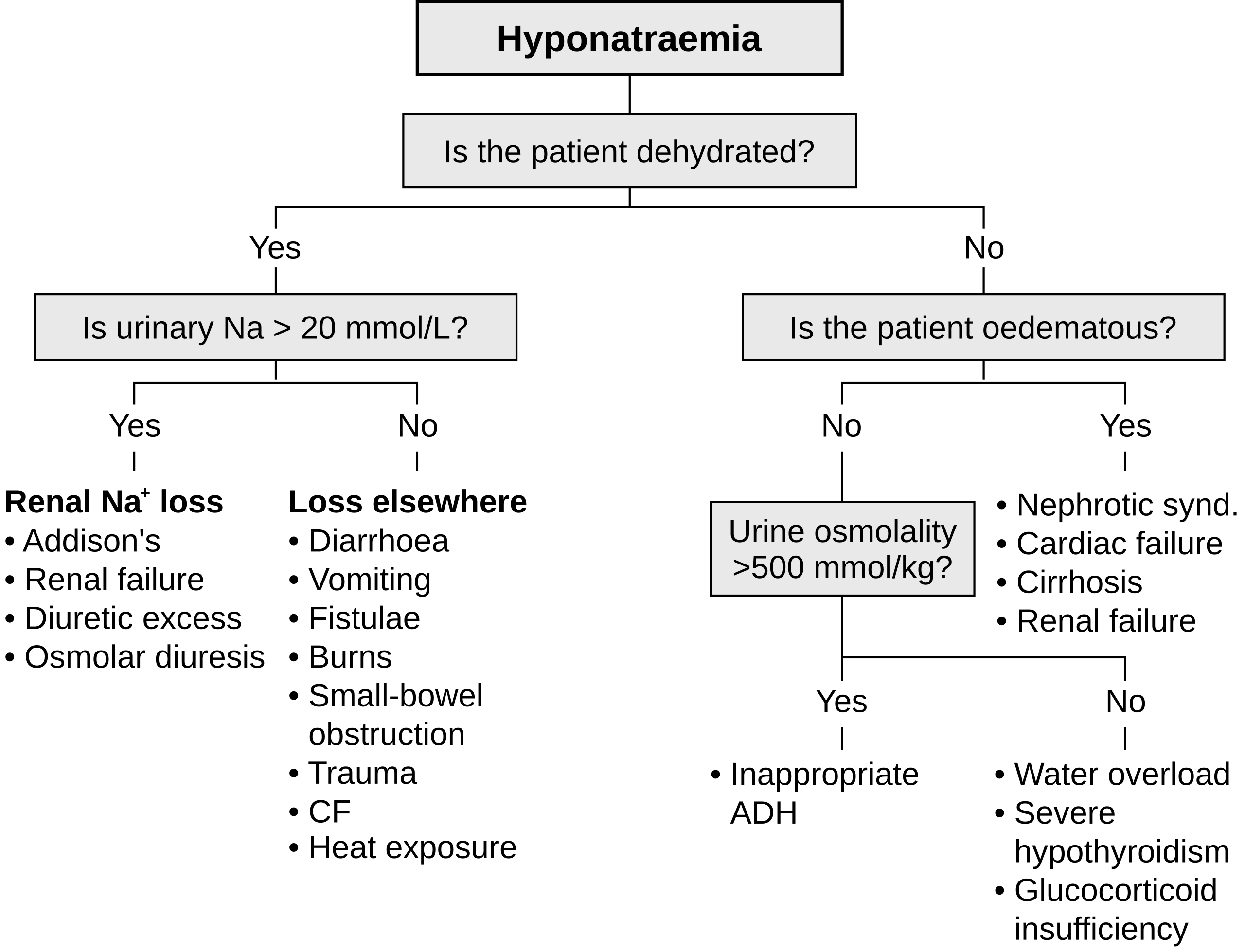
Hyponatremia noted → measure serum osmolality to confirm hypotonic hyponatremia (exclude pseudohyponatremia or hyperglycemia).
If hypotonic hyponatremia → assess patient's volume status (clinical exam) and check urine osmolality.
Urine Osm >100 mOsm/kg (not dilute) suggests ADH is present; if patient is euvolemic with urine Na >40 mEq/L, suspect SIADH (after ruling out hypothyroidism and adrenal insufficiency).
Diagnose SIADH → search for cause (evaluate for malignancy, CNS disease, medications) and address it (e.g., treat tumor or stop offending drug).
Manage SIADH hyponatremia based on severity: fluid restriction in most cases; use hypertonic saline for severe symptoms, and avoid rapid Na correction to prevent complications.
Heavy smoker with a new lung mass and hyponatremia (low Na, low serum Osm, high urine Osm) → SIADH from small cell lung cancer (ectopic ADH).
Post–head injury patient with confusion and hyponatremia, urine Osm 300 mOsm/kg → SIADH due to CNS trauma (inappropriate ADH release).
Elderly patient on an SSRI presenting with mild confusion and serum Na 125 mEq/L → drug-induced SIADH from an antidepressant.
Case 1
A 70‑year‑old man with a 60-pack-year smoking history is evaluated for headaches, confusion, and generalized weakness.
Algorithm of hyponatremia causes, distinguishing hypovolemic (dehydration), hypervolemic (edema-causing illnesses), and euvolemic causes like SIADH (ADH excess) and other endocrine etiologies.