X-linked recessive immunodeficiency caused by a BTK genemutation, resulting in failure of B cell maturation and near-absent immunoglobulins (agammaglobulinemia).
Classic pediatric primary immunodeficiency often tested on exams; fatal infections or organ damage can occur if not recognized and treated early (first immunodeficiency described, by Bruton).
Healthy for first few months of life (maternal IgG), then recurrent bacterial infections begin ~6–9 months (after maternal antibodies wane). Otitis media, pneumonia, sinusitis are common; infections often severe and require hospitalization.
Encapsulated bacteria like Streptococcus pneumoniae and Haemophilus influenzae are typical pathogens (due to lack of opsonizing Ig); also chronic diarrhea from Giardia (no IgA), and risk of severe enteroviral infections (e.g., polio, echovirus encephalitis).
Exam: absence of lymphoid tissue (tonsils, adenoids) and no lymphadenopathy (reflecting lack of B cells); spleen and liver typically normal (no lymphoid hyperplasia).
Suspect XLA in a baby boy with >1 serious bacterial infection after age 6mo; confirm with immunoglobulin levels and B-cell counts.
Labs: IgG, IgM, IgA all markedly low (often undetectable). Flow cytometry shows profoundly low CD19+ B cells (<2% of lymphocytes) with normal T cell number.
Physical exam clues: no palpable tonsils or lymph nodes suggests absence of B cells (seen in XLA).
Genetic testing for BTK mutation can confirm the diagnosis. A family history of males with early fatal infections may be present (X-linked recessive).
Avoid administering live vaccines (polio, rotavirus, MMR, varicella) in infants suspected of immunodeficiency until evaluation, as they can cause infection in XLA.
IgA is low (not all Igs); milder recurrent mucosal infections, often asymptomatic
Lifelong immunoglobulin replacement (monthly IVIG or weekly SCIG) to provide missing antibodies (significantly reduces infections).
Antibiotics for acute infections (aggressive therapy); consider prophylactic antibiotics to prevent recurrent sinopulmonary infections.
No live vaccines (e.g., oral polio, varicella); ensure siblings' vaccines are up-to-date to protect the patient (herd immunity).
Think Bruton's for B-cells (absent), Boys (X-linked), and infections starting at Babies age ~6 months.
No B cells → no Brainer: no tonsils! (Tonsillar tissue underdeveloped without B cells).
Recurrent severe infections in infancy, especially after 6mo, or vaccine-derived infection (e.g., from rotavirus or polio vaccine) → evaluate immune function (could be XLA).
Delayed diagnosis can lead to bronchiectasis from repeated pneumonias or chronic enteroviral encephalitis — start IVIG early to prevent organ damage.
Recurrent bacterial infections in male infant (>6mo) → suspect XLA.
Order quantitative Ig levels (expect pan-hypogammaglobulinemia) and lymphocyte immunophenotype (expect <2% B cells).
If Ig levels low + B cells absent → XLA likely; confirm with BTK genetic testing.
Begin IVIG replacement therapy promptly; treat active infections with appropriate antibiotics.
Avoid live vaccines; provide genetic counseling (X-linked inheritance).
8-month-old boy with recurrent otitis media, pneumonia (since 6 months) and absent tonsils → X-linked agammaglobulinemia (Bruton's).
Infant develops paralytic poliovirus infection after oral polio vaccine → suspect XLA (can't form antibodies to live vaccine).
Case 1
A 9-month-old boy has been hospitalized twice for pneumonia and skin abscesses. He also had recurrent ear infections since age 7 months.
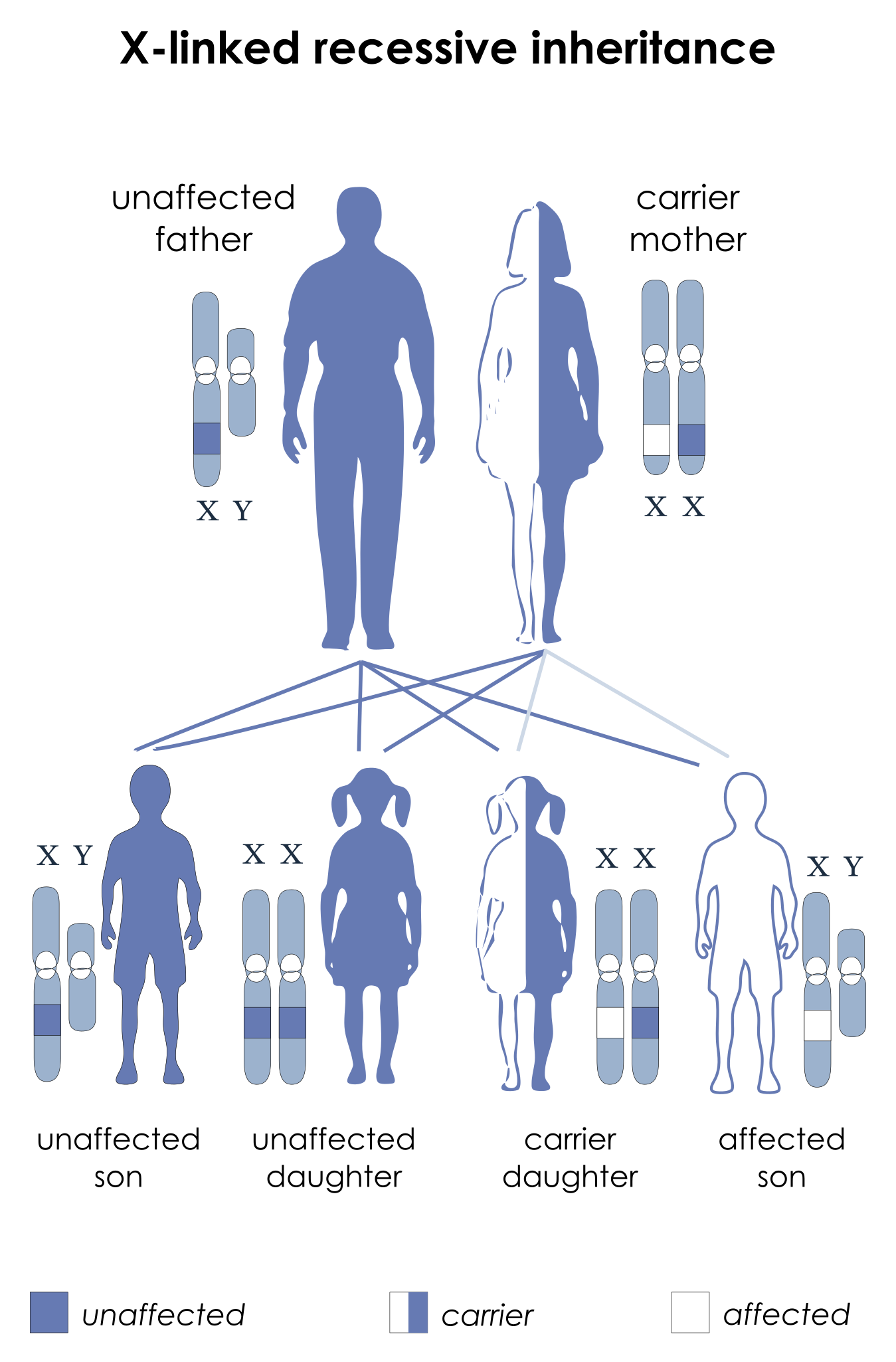
X-linked recessive inheritance pattern (carrier mother transmitting to affected son).