Injury of the lower brachial plexus (C8-T1 roots) causing paralysis of intrinsic hand muscles ('claw hand') and sensory loss in the medial arm/hand; often includes Horner syndrome if the T1 sympathetic fibers are affected.
Although much less common than Erb palsy, Klumpke palsy appears in exams to test brachial plexus anatomy. It signifies a lower trunk injury that can cause profound hand disability (and Horner syndrome in severe cases), highlighting the importance of recognizing nerve root levels and indicating the potential need for surgical intervention.
Newborn (obstetric) – Rare (<5% of brachial plexus birth injuries) but associated with breech delivery or arm traction during birth. Infant has a limp hand (no grasp reflex) with intact shoulder/elbow motion.
Adults – Occurs with forceful arm traction (catching oneself during a fall, pulling arm overhead). Presents as weakness/paralysis of the hand and forearm muscles with numbness along the ulnar side of forearm/hand.
Exam findings – Claw hand deformity (wrist extension, MCP hyperextension, IP joint flexion from intrinsic muscle paralysis) and sensory loss in C8-T1 dermatomes (medial forearm, ulnar hand). Reflexes: biceps/triceps intact (C5-7); grasp reflex absent in infants. Horner syndrome (ptosis, miosis ± anhidrosis) may accompany, indicating T1 sympathetic involvement.
Differentiate upper vs lower plexus: arm weakness plus hand clawing (with normal shoulder rotation/elbow flexion) points to a lower trunk (Klumpke) lesion, whereas an extended 'waiter's tip' arm indicates an upper trunk (Erb) lesion.
Check for Horner syndrome (ptosis, miosis) in suspected Klumpke palsy – its presence implies a preganglionic (root) avulsion of T1 with poor spontaneous recovery.
In an adult with Klumpke-like hand weakness and Horner signs *without* trauma, suspect a Pancoast tumor (apical lung tumor) compressing the lower plexus and sympathetic chain.
Condition
Distinguishing Feature
Erb-Duchenne palsy
upper trunk (C5-C6) injury – causes 'waiter's tip' arm (shoulder adducted, elbow extended) rather than claw hand
Thoracic outlet syndrome
compression of lower plexus (often by cervical rib) – causes lower trunk symptoms (ulnar hand numbness, intrinsic weakness) +/- vascular findings
Ulnar neuropathy
ulnar nerve lesion at elbow (cubital tunnel) causes clawing of 4th/5th digits and sensory loss in ulnar hand, but spares median-innervated fingers and has no Horner syndrome
Conservative (initial): Support and monitor. Begin passive range-of-motion exercises and physical therapy to prevent contractures while waiting for nerve recovery. Many neonatal injuries improve spontaneously within weeks to months.
Surgical: If no significant recovery by ~3–6 months (or sooner if signs of root avulsion), consult neurosurgery/orthopedics for possible nerve graft or transfer. Early surgical exploration is often recommended when Horner syndrome or complete palsy indicates avulsion.
After nerve repair or if residual deficits remain, provide long-term occupational therapy. Later orthopedic interventions (tendon transfers, muscle releases) can improve function in a chronically weak hand.
Klumpke = Klaw: lower trunk injury classically presents with a total claw hand (intrinsic minus hand).
Horner syndrome (ptosis & miosis in a hand palsy question) is a clue that it's a Klumpke (C8-T1) lesion with root avulsion.
Horner syndrome (ptosis, miosis on the affected side) accompanying a brachial plexus injury – suggests root avulsion with severe damage (spontaneous motor recovery <10%). This warrants early specialist referral.
No improvement in function over 3–6 months in an infant – signifies a more severe injury (e.g., neurotmesis) and the need for surgical evaluation. Also, any upper motor neuron signs (hyperreflexia, Babinski) indicate possible spinal cord involvement rather than an isolated plexus lesion.
Birth or trauma with arm weakness → Assess pattern: if hand is paralyzed with intact proximal arm, suspect Klumpke (C8-T1); if shoulder/elbow weak with intact hand, suspect Erb (C5-C6).
Perform detailed neuro exam: document muscle groups affected, sensory loss distribution, and look for Horner syndrome (implicates root avulsion). Consider imaging (MRI) if bone injury or avulsion is suspected.
Initial management for plexus injury is conservative: protect the limb, begin gentle PT/OT to maintain mobility, and closely monitor for return of function.
Reevaluate at ~3–6 months: if signs of reinnervation (improving strength) are present, continue conservative management; if no improvement, obtain electrodiagnostic studies and plan for surgical repair (nerve graft/transfer).
After surgical intervention or if late deficits remain, focus on rehabilitation and consider orthopedic procedures (e.g., tendon transfers) to optimize limb function.
Newborn with difficult breech delivery, now has a paralyzed hand (extended wrist, clawed fingers, no grasp) but normal shoulder movement ± Horner syndrome → Klumpke palsy (C8-T1 injury).
Adult who falls and grabs a ledge to avoid the fall, then develops intrinsic hand muscle paralysis with ulnar side numbness and ipsilateral ptosis → lower trunk brachial plexus injury (Klumpke).
Case 1
A newborn girl is delivered via breech extraction with noted arm traction. She has a limp left hand and does not move her fingers.
Case 2
A 25‑year‑old man falls from a tree and grabs a branch with his right arm to break the fall. Afterwards, he cannot move his right hand.
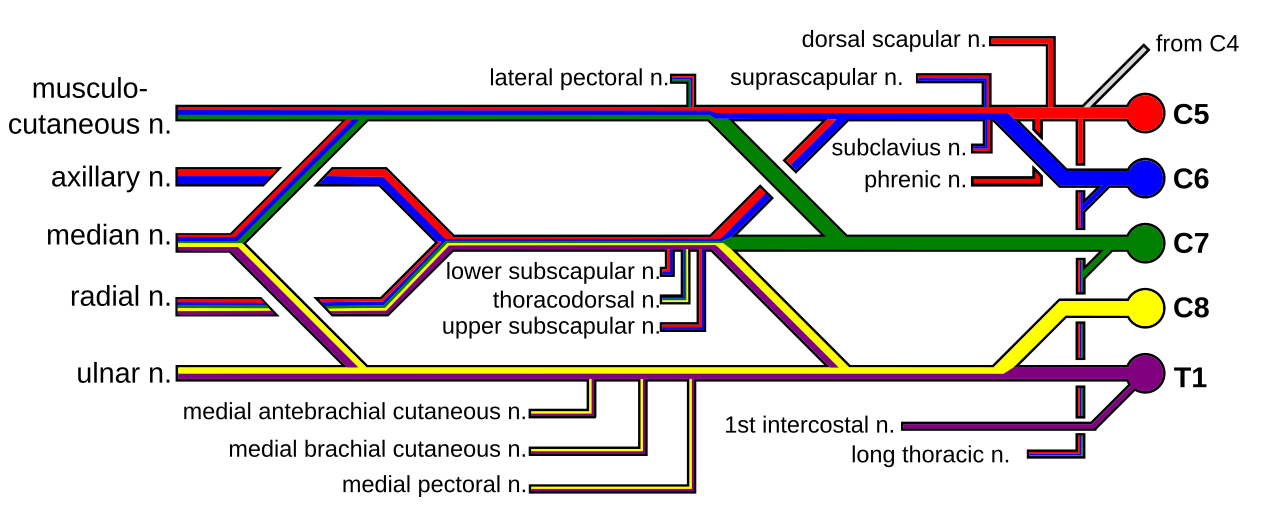
Color-coded diagram of the brachial plexus (C5-T1 nerve roots and branches) illustrating the lower trunk (C8-T1) involvement in Klumpke palsy.