An acute coronary syndrome marked by new or worsening chest pain (angina) at rest or with minimal exertion due to myocardial ischemia without infarction (no cardiac muscle cell death, hence normal troponin levels).
Represents an impending heart attack – unstable angina carries higher short-term risk of myocardial infarction and death than stable angina. Prompt recognition and treatment can prevent progression to an MI, making it a common emergency and exam topic.
Classically presents as chest pain at rest (often ≥10–20 minutes) or a crescendo pattern of angina (pain becomes more frequent, severe, or occurs with less exertion than before). The pain is typically a pressure or tightness, possibly radiating to the arm or jaw, and may come with diaphoresis, shortness of breath, or nausea – resembling an MI.
Electrocardiogram (ECG) often shows transient ST depression or T-wave inversions during episodes (signs of subendocardial ischemia), but no persistent ST elevation. Crucially, cardiac troponin levels are normal (by definition, no myocardial necrosis in unstable angina). Many patients have coronary risk factors (older age, smoking, diabetes, hyperlipidemia) or a history of stable angina that has now destabilized.
Initial approach: obtain a 12-leadECG and serial troponin levels in any patient with suspected ACS. If ST-elevation is seen → treat as STEMI (immediate reperfusion). If no ST-elevation, manage as NSTE-ACS (unstable angina/NSTEMI) while awaiting troponin results.
Distinguish unstable angina vs NSTEMI by biomarkers: if troponin elevates, it's an NSTEMI (myocardial infarction); if troponin remains normal, it's unstable angina. Both are treated similarly since both are non–ST-elevation ACS.
Begin treatment promptly: give aspirin (chewed) and relieve ischemia with nitroglycerin (sublingual or IV for ongoing pain) and β-blockers (unless contraindicated) to reduce oxygen demand. Provide oxygen only if hypoxic; use morphine for persistent pain.
Start antithrombotic therapy: administer an anticoagulant (e.g., IV heparin) and add a second antiplatelet (e.g., clopidogrel or ticagrelor) to aspirin. Also initiate a high-intensity statin as early as possible.
Consult cardiology and risk-stratify (e.g., TIMI or GRACE score). Patients with high-risk features (ongoing angina, heart failure, arrhythmia, hemodynamic instability) should undergo urgent cardiac catheterization (often within 24 hours) for possible PCI. Those stabilized without high-risk criteria can have noninvasive stress testing or elective angiography prior to discharge.
sharp, positional chest pain with pericardial friction rub; diffuse ST elevations on ECG (not a coronary syndrome)
All patients: aspirin immediately (unless contraindicated). Begin anti-ischemic therapy with nitroglycerin (sublingual or IV) for pain and a β-blocker within 24 hours to reduce cardiac workload (avoid β-blockers in cocaine-induced angina or severe bradycardia). Start high-intensity statin therapy early.
Dual antiplatelet therapy (aspirin + a P2Y₁₂ inhibitor like clopidogrel or ticagrelor) is standard to prevent clot growth. Also give anticoagulation (e.g., unfractionated heparin IV if an early invasive approach is planned, or enoxaparin for conservative management) to inhibit thrombus formation.
Monitor in a telemetry unit. If angina or ECG changes recur despite therapy, or patient has high risk indicators, proceed to urgent angiography for possible PCI (generally within 24 hours for unstable angina/NSTEMI). Otherwise, after stabilization, arrange for stress testing or elective angiography to guide further management prior to discharge. Ensure appropriate follow-up with long-term therapies (β-blocker, aspirin, statin, etc.).
No troponin, no infarction: unstable angina by definition has normal cardiac enzymes – if troponin rises, the diagnosis shifts to NSTEMI.
Think MONA-B for initial therapy: Morphine, Oxygen (if needed), Nitrates, Aspirin + β-blocker – the acute management for unstable angina/NSTEMI.
Unstable angina is often called "pre-infarction angina," a red flag that a coronary plaque is unstable and a heart attack may be imminent without intervention.
Chest pain that is ongoing despite treatment or new dynamic ST changes (or rising troponin) → signal progression to infarction; requires emergent reperfusion (consider urgent PCI).
Signs of cardiogenic shock (hypotension, cool clammy skin) or acute heart failure (e.g., pulmonary edema) during anginal episodes → indicate extensive ischemia. Also watch for ventricular arrhythmias (VT/VF) in ACS. These findings demand immediate aggressive management and transfer to a higher level of care.
Chest pain at rest or rapidly worsening angina → suspect unstable angina (ACS) and perform immediate ECG & troponin testing.
ECG results: ST-elevation → STEMI (activate emergency reperfusion). No ST-elevation → likely unstable angina/NSTEMI; continue ACS protocol and await biomarkers.
If troponin is elevated → NSTEMI (myocardial infarction) and continue ACS management. If troponin remains normal → unstable angina (high-risk ischemia without infarct) – manage aggressively as ACS because risk of MI is high.
Initiate acute treatment: MONA-B (Morphine, Oxygen if needed, Nitroglycerin, Aspirin, β-blocker) plus anticoagulation (e.g., heparin) and a second antiplatelet (clopidogrel or ticagrelor). Begin high-intensity statin therapy.
Perform risk assessment (e.g., TIMI score). Arrange for early invasive strategy (angiography ± PCI) if high risk or refractory symptoms. If low risk and pain-free, do stress testing to evaluate for ischemia before discharge. Ensure close follow-up for further outpatient management.
Middle-aged patient with chest pressure at rest (lasting ~15 minutes) and transient ST depressions on ECG, but normal troponins → unstable angina (acute coronary syndrome without MI).
Patient with a history of stable exertional angina now having chest pain at rest or with minimal effort, requiring more nitroglycerin to relieve → unstable angina (angina has become unpredictable/crescendo).
Case 1
A 62‑year‑old man with hypertension and hyperlipidemia, who has a history of stable exertional angina, now presents with chest discomfort at rest while watching TV.
Case 2
A 58‑year‑old woman with diabetes and coronary artery disease reports that over the past week her usual angina has become more frequent and now sometimes wakes her from sleep.
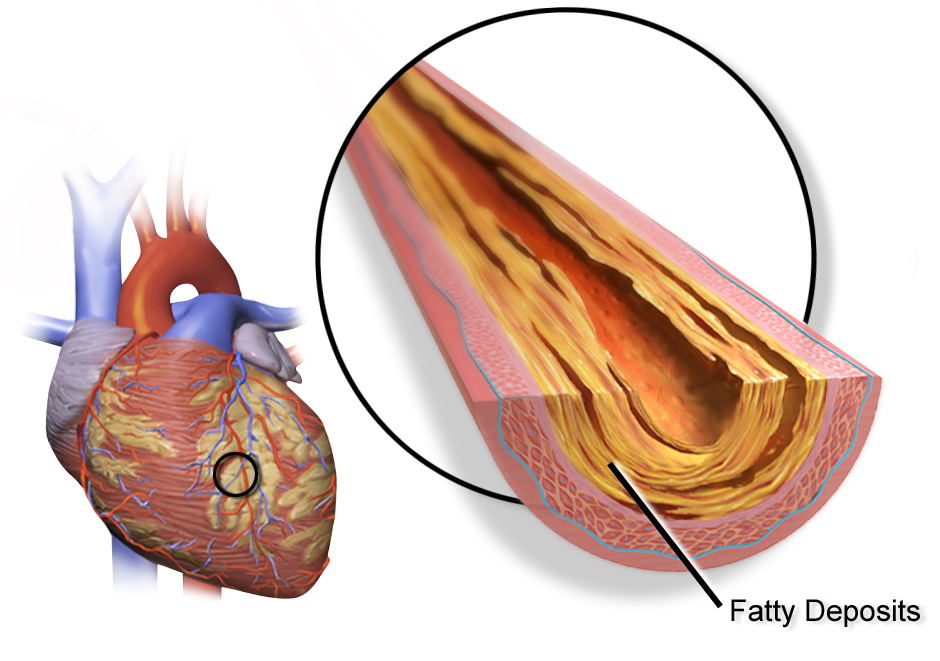
Cross-section of a coronary artery with a large atherosclerotic plaque (yellow fatty deposit) partially occluding the lumen, reducing blood flow.